When to See a Dermatologist for a Mole
Skin Moles are common. Almost everyone has a few, and some people develop hundreds. And melanoma, the deadliest type of skin cancer, can develop in or near moles.
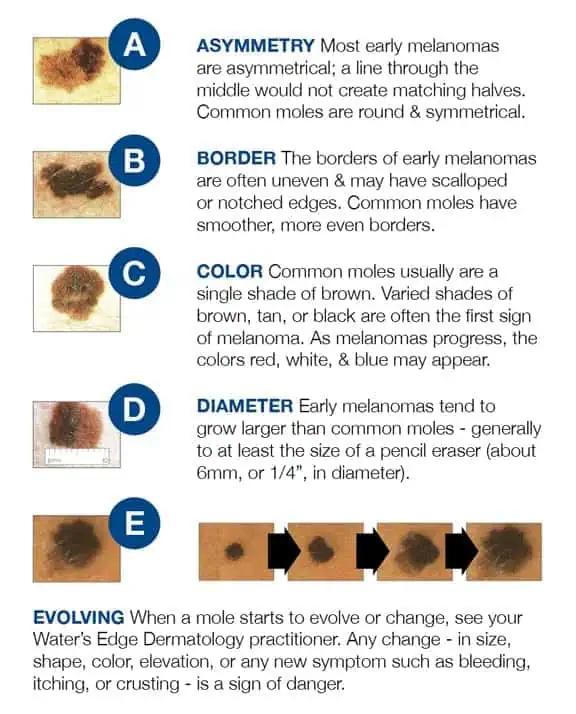
Don’t get frightened—most skin moles are not melanoma. So how do you know when to see a dermatologist for your moles? It’s easy; just keep in mind your ABCs.
A stands for ASYMMETRY: If one half of the mole is unlike the other half, have it looked at.
B stands for BORDER: If your mole has an irregular, scalloped or poorly defined border, it could be an early melanoma. Only a biopsy can provide conclusive results.
C stands for COLOR: If a mole’s color varies from one area to another, or if it turns shades of tan, brown and black (opposed to brown, which is normal), call your dermatologist.
D stands for DIAMETER: Melanomas are usually greater than 6mm (the size of a pencil eraser) when diagnosed, but they can be smaller. If a mole is large, have it examined and stay very aware of changes or growth.
E stands for EVOLVING: A mole or skin lesion that looks different from the rest or is changing in size, shape or color could be a sign of early skin cancer.
If you have a mole that shows any of these signs, be sure to schedule an appointment with a Water’s Edge Dermatology provider today. If something doesn’t seem right, or keeps grabbing your attention, come see us.

When it Comes to Staph Infections, Prevention is the Key
Different varieties of Staphylococcus aureus bacteria, commonly called "staph," exist. “Staph infections” are common and a term I remember hearing since I was a child; so this is not something new. Staph bacteria are normally found on the skin and in the nose of about one-third of the population. The bacteria are generally harmless unless they enter the body through a cut or other wound, and even then they usually cause only minor skin problems in healthy people. However, Methicillin-Resistant Staphylococcus Aureus (MRSA) is different. MRSA infections are caused by a strain of staph bacteria that's become resistant to the antibiotics commonly used to treat ordinary staph infections.
Most MRSA infections occur in people with questionable immune function who have been in hospitals or other healthcare settings, such as nursing homes and dialysis centers. When it occurs in these settings, it's known as healthcare-associated MRSA (HA-MRSA). HA-MRSA infections typically are associated with invasive procedures or devices, such as surgeries, intravenous tubing or artificial joints.
Another type of MRSA infection occurs in the wider community — among healthy people. This form, community-associated MRSA (CA-MRSA), often begins as a painful skin boil. It's spread by skin-to-skin contact. At-risk populations include groups such as high school wrestlers, child care workers and people who live in crowded conditions.
Staph skin infections, including MRSA, generally start as small red bumps that resemble pimples or boils. It is not uncommon for the patient to suspect a spider bite. These can quickly turn into deep, painful abscesses that require surgical draining. In most situations, the bacteria remain confined to the skin. But in the case of the HA-MRSA, they can also burrow deep into the body, causing potentially life-threatening infections in bones, joints, surgical wounds, the bloodstream, heart valves and lungs.
Antibiotic Resistance:
MRSA is the result of decades of unnecessary antibiotic use. For years, antibiotics have been prescribed for colds, flu and other viral infections that don't respond to these drugs. Even when antibiotics are used appropriately, they contribute to the rise of drug-resistant bacteria in part because they don't destroy every germ they target. In addition, patients who do not take their entire course of antibiotics also play a role in the emergence of these resistant strains. Bacteria live on an evolutionary fast track, so germs that survive treatment with one antibiotic soon learn to resist others.
Because hospital and community strains of MRSA generally occur in different settings, the risk factors for the two strains differ.
Risk factors for HA-MRSA:
- Being hospitalized. MRSA remains a concern in hospitals, where it can attack those most vulnerable — older adults and people with weakened immune systems.
- Having an invasive medical device. Medical tubing — such as intravenous lines or urinary catheters — can provide a pathway for MRSA to travel into your body.
- Residing in a long-term care facility. MRSA is prevalent in nursing homes. Carriers of MRSA have the ability to spread it, even if they're not sick themselves.
Risk factors for CA-MRSA:
- Participating in contact sports. MRSA can spread easily through cuts and abrasions and skin-to-skin contact.
- Living in crowded or unsanitary conditions. Outbreaks of MRSA have occurred in military training camps, child care centers and jails.
- Men having sex with men. Homosexual men have a higher risk of developing MRSA infections.
When to see a Healthcare Professional:
Keep an eye on minor skin problems — pimples, insect bites, cuts and scrapes — especially in children. If wounds become infected, seek medical care. Do not attempt to treat an MRSA infection yourself. You could worsen it or spread it to others.
What You Can Do:
Create a list that includes:
- Detailed descriptions of your symptoms
- Information about medical problems you've had
- Information about the medical problems of your parents or siblings
- All the medications and dietary supplements you take
- Questions you want to ask the doctor
What to Expect During Your Visit:
During your physical exam, your doctor will closely examine any skin lesions you may have. He or she might take a sample of tissue or liquid from the lesions for testing.
Both healthcare-associated and community-associated strains of MRSA still respond to certain antibiotics. In some cases, antibiotics may not be necessary. For example, your doctor, NP or PA may choose to drain a superficial abscess caused by MRSA rather than treat the infection with drugs.
Preventing HA-MRSA:
In the hospital, people who are infected or colonized with MRSA often are placed in isolation as a precaution to prevent the spread of MRSA. Visitors and healthcare workers caring for people in isolation may be required to wear protective garments and must follow strict hand hygiene procedures. Contaminated surfaces and laundry items should be properly disinfected.
Preventing CA-MRSA:
Wash your hands. Careful hand-washing remains your best defense against germs. Scrub hands briskly for at least 15 seconds, then dry them with a disposable towel and use another towel to turn off the faucet. Carry a small bottle of hand sanitizer for times when you don't have access to soap and water.
Keep wounds covered. Keep cuts and abrasions clean and covered with sterile, dry bandages until they heal. The pus from infected sores may contain MRSA, and keeping wounds covered will help keep the bacteria from spreading.
Keep personal items personal. Avoid sharing personal items such as towels, sheets, razors, clothing and athletic equipment. MRSA spreads on contaminated objects as well as through direct contact.
Shower after athletic games or practices. Shower immediately after each game or practice. Use soap and water. Don't share towels.
Sanitize linens. If you have a cut or sore, wash towels and bed linens in a washing machine set to the hottest water setting (with added bleach, if possible) and dry them in a hot dryer. Wash gym and athletic clothes after each wearing.
Most patients have come to know and often fear the term MRSA. However, when these infections are encountered the general community, in patients who are otherwise healthy, there is little to fear. Your healthcare provider will know exactly how to manage your condition and you are sure to recover without complication. Even so, it is still good behavior to practice the sound preventive measures we discussed above.

The Skinny on Tanning Beds and Skin Cancer Risk
As dermatology providers, we have often been asked the question from our patients as to the risks of indoor versus outdoor tanning.
Well, the answers have recently become clear and are alarming! The rise in skin cancer rates happen to coincide with the growth of indoor tanning, which was first introduced in the U.S. in the 1970s. Just one single indoor tanning session can increase users’ chances of developing the most serious form of skin cancer, melanoma, by 20%. Each additional session during the same year increases the risk almost another 2%.
These figures are based on a recent exhaustive analysis of 27 studies by the International Research Institute in Lyons, France. Essentially, people who tan indoors are 74% more likely to develop melanoma in their lifetime. Those who started tanning before age 35 have an even higher risk of 87%, of developing Melanoma. The majority of tanning beds patrons are girls and women ages 16 to 29. They display a high level of knowledge about the risks of UV exposure, but this awareness does not alter tanning behavior.
The number of melanoma cases has tripled in the past twenty years. In 2012, melanoma has affected an estimated 76,250 people, killing 9,180 in the U.S. alone. The British Medical Journal published a study linking more than 5% of all melanomas to tanning bed use.
Heredity can play a major role in melanoma, but the disease is often be triggered by intense, intermittent sun exposure. Fair-skinned people with light hair and eye color and those who have had sunburns or tend to burn easily are at increased risk of developing melanoma. So are those who have a family history of the disease or have ever themselves had a melanoma or other skin cancer. People with unusual-colored and large-sized moles are at a higher risk. In the earliest stages, melanoma is readily treatable. Left untreated, however, it can spread to vital organs and become life-threatening. Among patients with advanced disease, just 15% survive longer than 5 years.
Further studies have shown the role of indoor tanning on non-melanoma skin cancers. Close to 171,000 (or about 3%) of non-melanoma skin cancers diagnosed each year in the U.S. are attributed to indoor tanning. A single UV tanning session increases squamous cell skin cancers (SCC) by 67% and basal cell skin cancer (BCC) by 29%. Additionally, indoor tanners under the age of 25 double their risk of SCC and increase their risk of BCC by 40%.
Skin cancer prevention is optimally about sun protection. Nonetheless, secondary prevention involves early detection. An annual head to toe skin exam by a dermatology provider is recommended by the Skin Cancer Foundation, with a monthly self-examination. Familiarize yourself with suspicious appearing lesions, new or changing moles, spots, sores, lesions or growths. When patients are diagnosed and treated at an early stage of skin cancer, almost all make a full recovery.
Remember to wear sunscreen, apply 1 oz (2 TBS) to your entire body 30 minutes before going outside. Reapply every 2 hours or after swimming or excessive sweating.
Unfortunately, despite recent efforts to educate the public and limit young peoples’ access to indoor tanning facilities, sunbathing and indoor tanning have not significantly decreased. Thirty million Americans still visit indoor tanning salons, annually. Suntans and sunburns occur from overexposure to UV radiation, and both are signs of damage to skin cells. So, let’s get the word out there.
Learn more about skin cancer, or request a skin cancer screening at Water’s Edge Dermatology.
Sources
Publication of the Skin Cancer Foundation, Revised 2012
Robbins, Perry, M.D., The Numbers Add up:Just One Tanning Session Multiplies Skin Cancer Risk., Sun and Skin News, Winter 2012, Vol. 29, No.4
ReedK., BrewerJd Lohsce Cm, et al, Demierre MF, LazovichD, et al, Karagas MR, et al, Swerdlow AJ, Weinstock. Teen Tanners, The New Face of Melanoma, Skin Cancer Foundation Journal, Vol XXX, 2012, 34-37

Common Viruses of the Skin & What You Should Know
Common viruses of the skin include Molluscum Contagiosum, warts, and Herpes Simplex Virus Type 1 and 2. These viruses are common because they are contagious with skin to skin contact. Although most are only an annoyance, some do have the potential to cause harm to the person affected. Our goal at Water’s Edge Dermatology is to educate and alleviate any possible concerns of our patients.
Molluscum Contagiosum is a common skin condition, especially in children, that comes from the Poxvirus. The virus presents as small umbilicated blisters and is usually diagnosed by a trained eye but can be confirmed with a biopsy. Contagiosum is an adjective that well describes the condition because it is so contagious. Children have more skin-to-skin contact and a lower immunity than adults, explaining why it is more commonly seen at a younger age. There are treatments such as liquid nitrogen or Cantharone (a topical agent) that are often used if the condition is bothersome or spreading. Treatment is not necessary because Molluscum Contagiosum is not harmful and with time should go away on its own. This condition can be sexually transmitted, but more commonly is spread by touching or scratching the area. Helpful tips for prevention include: avoiding direct skin-to-skin contact, avoid sharing towels with someone who is infected, frequent hand washing and protecting the skin's barrier by keeping it well moisturized.
Warts are caused by a virus called the Human Papilloma Virus (HPV), which is easily transmitted. Warts are also more common is children because their immunity is lower than adults. Most often, warts are diagnosed by a trained eye but can also be confirmed by a biopsy. There are different types of warts including; common warts, flat warts, plantar (under the surface of the foot) warts, and genital warts. Treatment may be the same as for Molluscum Contagiosum and is also a condition that may resolve on its own. Warts are typically raised but can be flat as in the flat warts or on the plantar surface of the foot. If warts are found in the genital region, they are usually considered to be sexually transmitted. However, common warts can also be transferred to the genitalia. Warts can be eradicated with treatment but they can return. Women who have a partner diagnosed with genital warts are at a higher risk for cervical cancer and should have regular pap smears. Helpful tips for prevention include: frequent hand washing; avoiding skin-to-skin contact with affected areas; wearing shoes in locker rooms, water parks, public pools and public showers to protect the feet; and protecting the skins barrier by keeping it well moisturized.
Herpes Simplex Virus (HSV) has two types (I and II), that when active, present with blisters or sores that can be painful. Type I is the cold sore virus and is generally found on the face, and type II is the sexually transmitted virus that is typically found in the genital area. However, type I has been found in the genitalia and type II has been found in other parts of the body. Once exposed to the virus, it may lay dormant for a long period of time, or may be such a mild case making it difficult to identify the source of infection. Stress and sun exposure can activate the dormant virus. HSV is contagious during flares but can also be contagious when no lesions are present. HSV is most commonly diagnosed by a trained eye, but a viral culture or blood work can be taken to confirm the diagnosis. HSV is treatable but there is no cure. Symptoms that may indicate the virus is active include tingling, itching, tenderness or burning sensation in the affected area. The treatment is antiviral medications like acyclovir or valacyclovir. If the medication is taken at onset, the symptoms may be minimized and the duration may be shortened. The symptoms will go away on their own with no treatment but may take longer than with the medication. Tips for prevention include: avoiding skin to skin contact to the affected area of a person with known HSV and avoiding sharing drinks, towels, lip balms or other products that may come in contact with the affected area.
These are some of the most common viruses of the skin but certainly not all of them. The key is early diagnosis and prompt treatment for any condition. Proper hand washing may not prevent these conditions, but is the number one way to avoid spreading infections. If you have any questions, please fill free to contact any of our offices. We are happy to help you in any way we can.
Mohs Surgery for Skin Cancer Treatment
Skin cancer is the most common type of cancer in the United States. And skin cancer rates are increasing in all races across the country.
At Water’s Edge Dermatology, our specially trained providers perform Mohs Surgery to treat skin cancer. Mohs micrographic surgery is a specialized, highly effective technique for the removal of skin cancer that is practiced throughout the world.
Here’s what Water’s Edge Dermatology patients are saying about Mohs Surgery.
Mohs Surgery permits the immediate and complete microscopic examination of the removed cancerous tissue, so all “roots” and extensions of the cancer can be eliminated. Due to the methodical manner in which tissue is removed and examined, Mohs surgery has been recognized as the skin cancer treatment with the highest reported cure rate.
Talk to your Water’s Edge Dermatologist about Mohs Surgery, or schedule your appointment for a skin cancer screening today.
Learn more about the types of skin cancer and skin cancer treatments.